Prenatal Counseling · Atlanta Perinatal Associates
High-Risk NIPT Result
22q11.2 Deletion Syndrome
22q11.2 Deletion Syndrome
What this result means — and what comes next
Screening Result · Not a Diagnosis
What Is NIPT?
Understanding the test you had
🩸
Source
Maternal Blood
Analyzes cell-free fetal DNA circulating in your bloodstream
🔬
What It Detects
Risk Probability
Estimates the likelihood of certain chromosomal differences — not a definitive answer
📊
Result Type
High Risk
"High risk" means elevated probability — it does not confirm a diagnosis
✅
NIPT is a screening tool. A high-risk result is the beginning of a conversation, not a final answer.
What Is 22q11.2 Deletion Syndrome?
Also known as DiGeorge or Velo-Cardio-Facial Syndrome
🧬
What Happens
A small piece of chromosome 22 is missing
This region (22q11.2) contains genes important for heart, immune, and brain development
👶
How Common
~1 in 4,000
The most common microdeletion syndrome — more common than many well-known conditions
Key Concept
22q11.2 DS is highly variable. Even within the same family, one person may have mild learning differences while another has a heart defect. No two cases are identical.
What Does "High Risk" Really Mean?
Positive Predictive Value (PPV) by clinical scenario
| Clinical Scenario | Estimated PPV | Interpretation |
|---|---|---|
| General population · No ultrasound findings | ~18–19% | Roughly 4 in 5 results are false positives |
| Updated algorithm / specific platforms | ~40–53% | About half of positive results are confirmed |
| Ultrasound anomalies present | 50–75% | Higher likelihood when structural findings coexist |
⚠️
Important: Pregnancy decisions must never be based on NIPT alone. Confirmatory testing with chromosomal microarray (CMA) is required.
Sources: Dar et al. AJOG 2022 · Cong et al. Sci Reports 2025 · Soster et al. Front Genetics 2023
Why False Positives Occur
Three main sources of a misleading result
👩
Maternal Carrier
Unrecognized maternal deletion
In ~⅓ of false positives, the mother herself carries the deletion — often undiagnosed
🧩
Placental Mosaicism
Placenta ≠ Fetus
The deletion may be present only in placental cells, not in the fetus itself
⚙️
Technical Factors
Laboratory variation
Different NIPT platforms use different methods; SNP-based vs. counting methods are not equivalent
💡
A false positive does not mean the test was wrong — it means confirmatory testing is essential before drawing conclusions.
Confirmatory Diagnostic Testing
The only way to know for certain
🔬
Preferred Test
Chromosomal Microarray (CMA)
Identifies all deletions, determines deletion size, and detects other chromosomal differences
🏥
How Obtained
Amniocentesis or CVS
Amniocentesis preferred after 15 weeks · CVS available in first trimester · Or postnatal testing
1
Genetic Counseling Referral
Discuss testing options, risks, and implications in detail with a certified genetic counselor
2
Invasive Testing (Amniocentesis / CVS)
CMA performed on amniotic fluid or chorionic villi — provides a definitive answer
3
Parental Testing (if fetal deletion confirmed)
Both parents offered CMA or FISH to determine if deletion is inherited or de novo
Prenatal Imaging Workup
Recommended regardless of whether confirmatory testing is pursued
🫀
Fetal Echocardiogram
Cardiac Anatomy
Conotruncal defects are the most strongly associated ultrasound finding — present in ~60–75% of confirmed cases
🔭
Detailed Anatomy Scan
Level II Ultrasound
Evaluates for renal anomalies, palate, thymus, and other structural markers associated with 22q11.2 DS
Clinical Note
Approximately half of pregnancies with a positive NIPT result will show ultrasound findings at some point. A normal ultrasound does not rule out the deletion.
ACMG Guideline 2023 · Blagowidow et al. Genes 2023
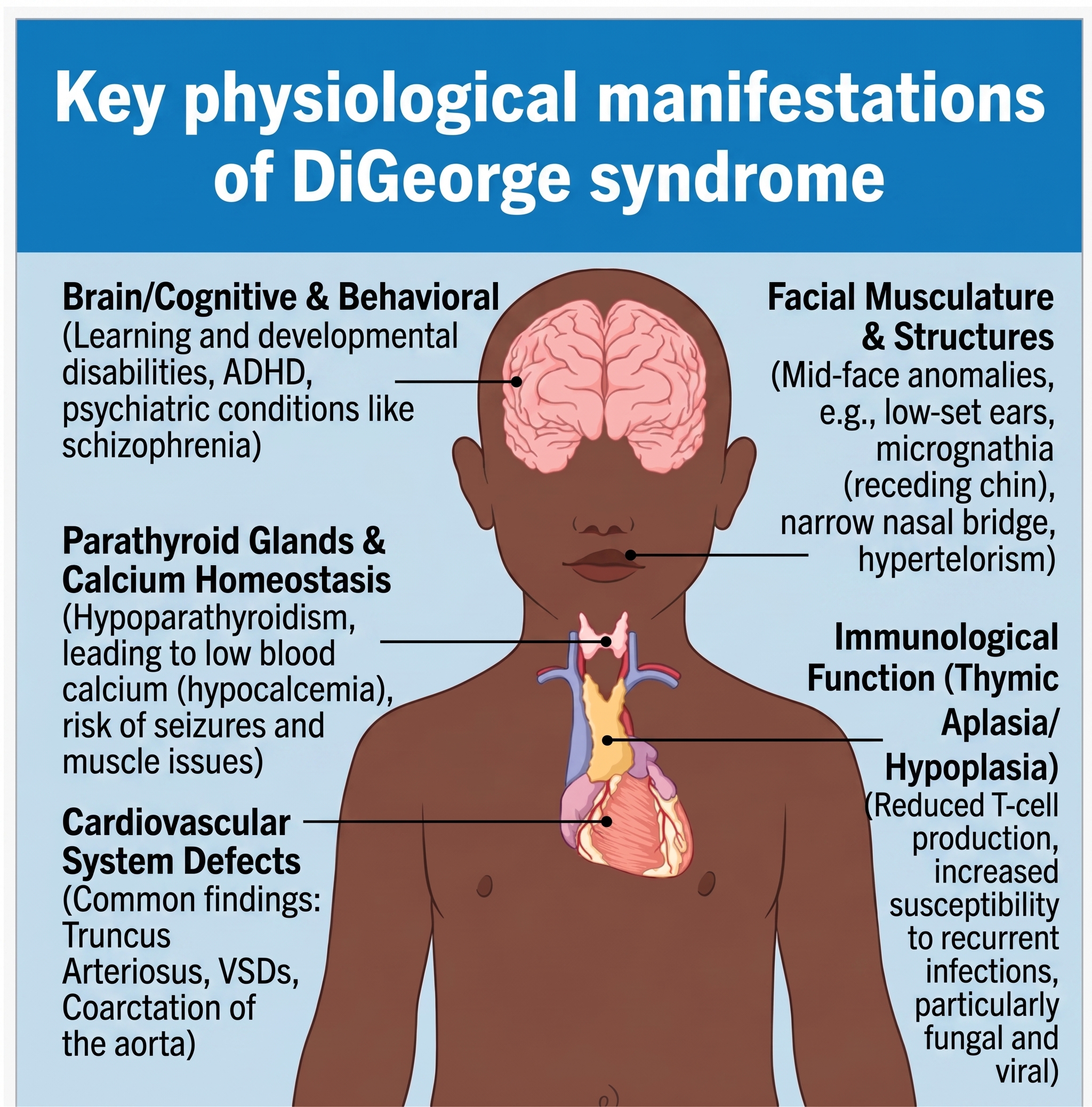
If the Deletion Is Confirmed
Possible features — highly variable; not all will be present
🫀
Heart
Conotruncal defects in 60–75%
(Tetralogy of Fallot, truncus arteriosus, interrupted aortic arch)
(Tetralogy of Fallot, truncus arteriosus, interrupted aortic arch)
🛡️
Immune System
Thymic hypoplasia → T-cell deficiency → increased infection risk
👄
Palate
Cleft palate or velopharyngeal insufficiency → feeding difficulties, speech
🧪
Calcium / Parathyroid
Neonatal hypocalcemia → possible seizures; hypoparathyroidism
🧠
Neurodevelopment
Developmental delays, learning differences; 25–30% lifetime risk of psychiatric illness
🌈
Variability
Spectrum ranges from mild learning differences to significant medical needs — outcomes cannot be predicted prenatally
Inheritance & Recurrence Risk
Understanding how this can happen in families
De Novo (New Mutation)
>90% of cases
The deletion occurred spontaneously — neither parent carries it. Future pregnancy recurrence risk is <1%.
Inherited from a Parent
~10% of cases
If a parent carries the deletion, each pregnancy has a 50% chance of inheriting it (autosomal dominant).
Maternal Source
~⅓ of false positives
A positive NIPT may reflect an unrecognized maternal deletion rather than a fetal one. Maternal testing is recommended.
Parental Testing
CMA or FISH
If fetal deletion is confirmed, both parents should be tested to determine inheritance pattern and guide future family planning.
Multidisciplinary Care Plan
If the deletion is confirmed prenatally
1
Maternal-Fetal Medicine (MFM)
Continued surveillance with serial ultrasounds and coordinated care planning throughout pregnancy
2
Pediatric Cardiology
Prenatal cardiac consultation; plan delivery at a center equipped for neonatal cardiac stabilization if needed
3
Medical Genetics
Comprehensive counseling on phenotypic spectrum, parental testing, and long-term management expectations
4
Neonatology / Neonatal ICU Planning
Anticipatory guidance for neonatal hypocalcemia monitoring, immune evaluation, and feeding support
Your Next Steps
A clear path forward — one step at a time
🧬
Step 1 — Confirm or Rule Out
Genetic Counseling + CMA
Schedule genetic counseling. Discuss amniocentesis (or CVS) with chromosomal microarray for a definitive answer.
🔭
Step 2 — Imaging
Detailed Ultrasound + Echo
Level II anatomy scan and fetal echocardiogram to evaluate for structural findings.
👩👨
Step 3 — Parental Testing
If Fetal Deletion Confirmed
Both parents offered CMA or FISH to determine if deletion is de novo or inherited.
🤝
Step 4 — Team Support
You Are Not Alone
Your care team — MFM, genetics, cardiology — will guide every decision together with you.
🚫
No irreversible pregnancy decisions should be made based on this screening result alone. Diagnostic confirmation is essential first.
🤝
We Are Here With You
A high-risk NIPT result raises important questions — but it is the start of a process, not an answer.
Your care team will walk with you through every step: confirmatory testing, imaging, specialist consultations,
and planning for the healthiest possible outcome.
ACMG Guideline 2023
Dar et al. AJOG 2022
Scheuerle et al. Pediatrics 2025
Blagowidow et al. Genes 2023
Atlanta Perinatal Associates · Dr. Chukwuma Onyeije, MFM